")
This story was told to CreakyJoints by Kara N. Corps, DVM, PhD, Dipl. ACVP, Director of Comparative Pathology & Digital Imaging Shared Resource at The Ohio State University College of Veterinary Medicine. As a result of immunotherapy treatments for triple negative breast cancer, Kara experienced irAEs — immune-related adverse events, an emerging area of study observing the potential side effects of immunotherapy. Kara tells her story and offers advice for others with this trifecta of conditions who may find it difficult to know where they “fit.”
My Cancer Diagnosis Story
In September 2021, I was doing my regular monthly breast self-exam and found a lump. It wasn’t very big, but because I’m a pathologist, I knew immediately it was not good.
That started a weeks-long journey of getting in to see a doctor, having a mammogram, getting a biopsy, and shortly after, receiving the diagnosis of triple negative breast cancer. It was replicating quickly, which was both good and bad: That meant it was growing fast, but that there was a reasonably good chance I was going to respond to chemotherapy.
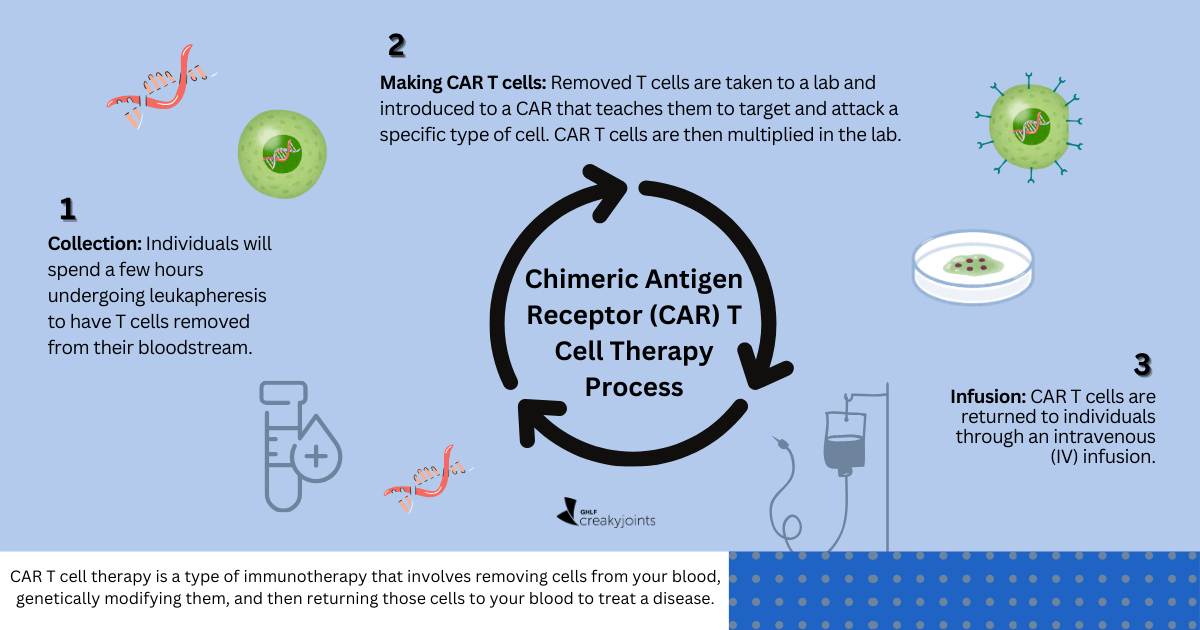
From the day I found the lump to when I started chemotherapy, it had grown more than four centimeters in not even a month and a half. I did a typical chemotherapy regimen for triple negative breast cancer, which was 12 weeks of carboplatin-Taxol. During that time, I started the immunotherapy, pembrolizumab (Keytruda), that I eventually got five doses of — and that sort of kicked off the whole duality journey.
I got one round of chemo starting in early November 2021, then I started the immunotherapy during my next dose of chemotherapy, which was one week later. Because of my background, I already knew that immunotherapies were being used in a lot of different kinds of solid tumor cancers, including breast cancer.
Before my treatment, I walked in the door with the concern that I had a preexisting autoimmune condition. This condition was never definitely diagnosed, which is super common in autoimmune patients, but we always considered it lupus-like. My symptoms include joint and muscle pain, swollen joints, hair loss, depigmented skin, and chronic fatigue. I’ve had it since I was in my late teens.
However, I happened to find an oncologist who’s considered a leading expert in immunotherapy use in breast cancer patients. She’s amazing and frighteningly intelligent, while also having one of the best bedside manners I’ve ever seen. She showed me a lot of her own data on the immunotherapy trials that she had.
What Happened When I Started Immunotherapy
The impact of my immunotherapy didn’t happen immediately. I was only getting the pembrolizumab every third visit. The first time I got it, I had a bit of an increase in joint pain and swelling that night — but that’s not necessarily unexpected. Lots of patients report that.
Then, I got a bit of a skin rash, which was pretty diffused all over the place. Most of my arms and legs were covered, but it cleared up right away, so no big deal.
However, the next time I went in to get my immunotherapy infusion, I got home, was sitting on the couch eating dinner, and I reached up to an eight out of 10 level of pain in my right knee. All of my joints were a little painful, but that right knee was in particular. I spiked a low-grade fever, which isn’t uncommon with immunotherapy. It went away within the first 24 hours.
But then, with my third dose, the crushing pain started again in my right knee — and my other joints were worse than they had been in the past. I went to bed, and at 2 am in the morning, I woke up with a pounding heartbeat and just couldn’t warm up. We grabbed a thermometer and I had a really high fever. When you’re on chemo, they tell you to call in immediately if you spike a high fever.
They told me to come in and admitted me right away, pumping me full of fluids and anti-inflammatories. It took them about two and a half hours to get that fever under control, which had spiked up to around 102 degrees Fahrenheit that time.
I also had a rash again that was clearly inflammatory. You could watch it move in my skin, up and down my legs and arms, which was creepy. My heart rate had gone up to about 130 to 140 at rest. When you’re on chemo, the knee jerk assumption of anyone who spikes a fever is that they could potentially be septic, so I was in the hospital for five days and pumped with antibiotics.
Eventually I went home — but we repeated that pattern four more times after immunotherapy. The doctors started looking for causes, like a random respiratory virus.
However, I kept getting the immunotherapy, and that’s where the whole cancer-autoimmune patient thing really started to become difficult mentally. It’s like, yes, I want you to kill the cancer. I would rather get immunotherapy since that’s a cutting-edge way of preventing the cancer from causing bigger problems or spreading.
By late April 2022, I was done with chemo, but still getting immunotherapy. I was scheduled for surgery, but one morning I got up and wasn’t appropriately coherent. My systolic blood pressure was 70 and I shouldn’t have been conscious. At the clinic they pumped me full of fluids and said they should postpone my surgery — which, as a cancer patient, is the last thing you want. At that point you’re like, okay, we’ve hammered it with all these meds and now I just want whatever’s left out.
They told me to come back the next day for another immunotherapy dose and to rest for several more weeks before going into surgery. Like clockwork, I had symptoms again in the middle of the night, except this time it was exponentially worse. My heart rate was between 170 and 200 at rest and my fever was over 104. I was held in the ER overnight.
I experienced cardiac damage from the high heart rate. My whole heart was inflamed because of the immunotherapy. We explored a number of different things, but basically, it came down to either we’re causing a massive cytokine storm [immune overreaction] or I’m having an autoimmune situation that is systemic, associated with the immunotherapy.
Making the Difficult Decision to Stop Immunotherapy
Eventually we determined it was associated with immunotherapy, and I was torn again. This drug was my best option for a long-term, disease-free survival from cancer, but it was also putting my life at risk.
We decided we needed to discontinue it at that point. Again, I was upset, and I think anyone would be. But that was a smart move on everybody’s part, because after they discharged me from hospital, I ran a fever for eight weeks. They were treating me with over-the-counter anti-inflammatories every four-hours.
I finally had surgery, a double mastectomy, and gradually that fever went away. The biopsy or post-op pathology came back and they couldn’t find solid mass. They could find a very small number of cells remaining that were identifiable as tumor cells, so they would not call that a complete response, even though there was barely anything left. We did 24 weeks of oral capecitabine, a type of chemotherapy.
The Lingering Effects of Immune-Related Adverse Effects
To this day, I still have ongoing side effects from the immunotherapy. The joint stuff is still there. If my day-to-day pain prior to this whole cancer journey with my original autoimmune condition was a one, my normal baseline now is a three to a four on a good day.
On a bad day, it’s much worse. I have ongoing, severe dry eye and for a time had double vision. Now we see in the literature that there have been a handful of patients who have reported very similar things. They think it’s associated with a neuromuscular inflammation induced by the immunotherapy. Luckily for everybody, from at least all the reports I have seen, it’s always been temporary — like it was for me.
Now it’s just about monitoring myself and seeing the doctor every three months. The weird silver lining is that because I’d had an autoimmune condition for so long, I was already very good at writing down symptoms and cataloging them so that I had a record of them to talk to my doctors about.
Surprisingly, it wasn’t difficult for me to tell the difference between my autoimmune disease and the immune-related adverse effects. We think of pain as pain — or fatigue as fatigue — but they were so drastically different between the two. Can I explain to you exactly what they feel like and why I know they’re different? No, but they’re totally different.
That said, when I have a flare of the autoimmune symptoms, it’s way worse than it used to be. Instead of just being a dull ache, now I get throbbing aches with sharp, stabbing pains to the point that it’s disruptive. I’ve had joint pain post-immunotherapy that is bad enough that I have to stop and sit down and wait for it to pass because I can’t do anything else.
What I Would Tell Other Patients
Knowing what I know now, if somebody came to me and said, “I’m going to go on immunotherapy, on the same drug you were on for the same kind of cancer,” I would tell them that I don’t think there’s anything that I could go back and do differently.
You can have a patient who had no autoimmune stuff walk in and get one of these meds and end up with a side effect. People’s immune systems and what they’re going to do when they get a checkpoint inhibitor are going to differ. There are patterns, but that doesn’t mean everybody’s going to present the same.
The Internet can be a dangerous dark hole. Don’t go down the dark holes, because that’s not good. It just makes you more afraid. You already have cancer and you don’t need to be more afraid. But ask your doctors if there are other patients going through similar things who you can talk to for advice. Seek out other patients to talk to.
Trying to balance turning on your immune system to fight your cancer — but not making your life more difficult as a result — is a hard thing to do. The doctors don’t have all the absolute right answers and neither does anybody else. However, if you’re able to say what you’re feeling and what you think you need, that’s really important.
A patient does not need the medical training I have to know something is wrong. They live in their own bodies, and if they think something is wrong, they have every right to have a dialog with their health care team about it. Part of the job of an oncology team is to listen and take their concerns seriously.
I’m cancer-free at this point and managing symptoms, training my grad students, working too many hours, and having fun. Remember, if you do go through a situation like mine, that doesn’t mean that you’re stuck in a bad place — because I’m not in a bad place anymore.
Be a More Proactive Patient with PatientSpot
PatientSpot (formerly ArthritisPower) is an app and website made for people living with chronic conditions. You can track your symptoms and treatments, access support resources relevant to your needs, and choose to participate in research to help advance the understanding of chronic diseases. Learn more and sign up here.