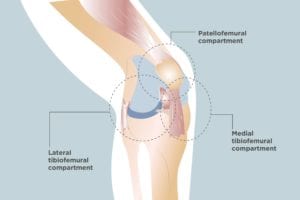
You or a loved one may have been diagnosed with osteoarthritis in the knee, but there’s more to the diagnosis than just that. When it comes to knee osteoarthritis, there’s meaningful variation in how much of the knee joint is affected. The knee is a complex joint that contains three compartments that have their own functions and structures — and any or all of them can be affected by OA. They are:
Medial femoral-tibial compartment, the inner part of the knee where the tibia (shinbone) meets the femur (thigh bone)
Lateral femoral-tibial compartment, the outside part of knee where the tibia (shinbone) meets the femur (thigh bone)
Patellofemoral compartment, the joint between the kneecap and the end of the femur (thigh bone)
The medial femoral-tibial compartment is the part of the knee that is most commonly affected in cases of osteoarthritis. When all three components of the knee are affected, a patient is diagnosed with tricompartmental osteoarthritis.
Tricompartmental Osteoarthritis Symptoms
The signs of OA of the knee are similar regardless of the number of compartments affected. Symptoms of knee osteoarthritis include:
- Knee pain
- Knee stiffness: Usually worst in the morning and after sitting for long periods of time, but it typically eases up within an hour
- Swelling
- Trouble bending or straightening the leg
- Difficulty going up and down stairs
- Crepitus: The medical term for sounds like grinding, popping, crunching, etc. your knee may make (they’re harmless)
- Weakness or buckling of the knee
- Bow-legged or knock-kneed gait and appearance
One symptom that may be more commonly seen in people with tricompartmental osteoarthritis compared with other kinds of knee arthritis is loss of proprioception, or the ability to know where your body is in space. “This hasn’t been proven, but patients who have tricompartmental OA may lose more muscle strength, which could lead to weakness and problems with proprioception,” says Kathryn A. Miller, MD, medical director for the Knee and Hip Comprehensive Non-Surgical Osteoarthritis Management Clinic at University of Wisconsin Health at The American Center.
Proprioception allows you to move your limbs without looking at them. It’s how you can step onto a curb without looking at your feet, for example. If you’re experiencing loss of proprioception due to tricompartmental osteoarthritis, you may find yourself stumbling and tripping more often.
Causes and Risk Factors for Tricompartmental Osteoarthritis
Little is known about what makes someone susceptible to tricompartmental OA because researchers still have a great deal to learn about the condition. It’s not even clear how commonly this type of osteoarthritis occurs, Dr. Miller says.
Experts do know that osteoarthritis can be caused by years of wear and tear or result from an injury to the knee. Other risk factors for knee osteoarthritis include smoking, genetics, and obesity.
In Dr. Miller’s experience, people with tricompartmental OA are more likely to have developed the condition from lifestyle issues or genetics.
“Someone who developed knee osteoarthritis from an injury, for example, may have hurt just one part of their knee, so that’s the only compartment affected,” she says. “Whereas tricompartmental OA may be due more to a genetic factor or some other process like obesity or smoking that is causing more uniform damage throughout the joint.”
How Doctors Diagnose Tricompartmental Osteoarthritis
While it might seem like imaging tests such as X-rays would be the definitive way to identify tricompartmental osteoarthritis, Dr. Miller says these tests are actually of limited use. That’s because the signs of OA — narrow spacing between the joints due to loss of cartilage and the formation of osteophytes (bone spurs) — may not appear on an X-ray until a person’s osteoarthritis has become severe.
Instead, your doctor will rely more on family history, symptoms, and the results of a physical exam. The exam may include:
- Range-of-motion tests
- Feeling the affected joint for signs of OA such as tenderness and bony lumps
- Evaluating posture and gait
X-rays are frequently ordered, but your doctor may also request a more advanced test such as an MRI if they are uncertain of your diagnosis.
Primary care doctors can diagnose and manage tricompartmental osteoarthritis, though some may prefer to refer you to an orthopedic surgeon, rheumatologist, or sports medicine doctor.
Treatment for Tricompartmental Osteoarthritis
For some patients, over-the-counter pain medication such as ibuprofen or acetaminophen may be enough to manage the symptoms of tricompartmental osteoarthritis. If not, your doctor may recommend prescription-strength anti-inflammatory medication, which is available in oral and topical forms.
While corticosteroid injections and injections of hyaluronic acid (which mimics the cushioning of cartilage) can be helpful, Dr. Miller says doesn’t like to rely on them often. “They’re fine to use once in a while, but I’d rather not have patients come in every three months to get injections when they could manage their pain with oral and topical medication and lifestyle changes,” she explains.
Lifestyle changes that benefit tricompartmental OA patients include losing weight if you’re overweight or obese, exercising (a physical therapist can help you get started), and quitting smoking if you smoke.
One thing that’s usually helpful for OA, but *not* for tricompartmental OA is wearing devices like braces.
“These are helpful if only one part of the knee if affected because they’re designed to isolate and take pressure off that one part,” Dr. Miller says. “A brace won’t do anything for someone who has OA in all three compartments. It could actually make the OA in the other two compartments worse.”
Undergoing a total knee replacement is an option for people with tricompartmental OA, though surgery is best reserved for those who aren’t helped by medication and lifestyle changes. But people should stick to these less invasive treatments for a sufficient amount of time before declaring them a failure, she says: “If you haven’t improved after four to six months, then I’ll feel more confident recommending a total knee replacement.”